COVID-19 and the endocrine system
- A novel coronavirus disease (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has affected millions in over 200 countries worldwide. Although COVID-19 can be asymptomatic, the primary presentation in symptomatic patients is in the form of viral pneumonia, sometimes complicated by acute respiratory distress syndrome and/or sepsis. In addition, myocarditis and acute kidney injury have also been described in COVID-19. On the contrary, endocrinological manifestations have not yet been reported in patients with COVID-19.
- The pathogenesis of COVID-19 entails entry of SARS-CoV-2 via the respiratory system and lodgement in the lung parenchyma. Thereafter, it uses angiotensin-converting enzyme 2 (ACE2) as a receptor for ingress into host pneumocytes. In addition, the viral ribonucleic acid (RNA) has also been detected in the plasma or serum of COVID-19 patients, suggestive of viremia . This implies that apart from pneumocytes, the virus is freely available to interact with ACE2 expressed in other tissues. As a matter of fact, a number of endocrine organs do express ACE2, namely pancreas, thyroid, testis, ovary, adrenal glands and pituitary. Hence one could expect endocrine repercussions due to interaction of SARS-CoV-2 with ACE2 expressed on these organs. However, based on observations drawn partly from studies pertaining to the prior SARS outbreak (in 2003) and partly from animal models, we aim to explore the possible effects of COVID-19 on the endocrine system.
COVID-19 and endocrine pancreas
- ACE2 is expressed in pancreas with mRNA levels being higher in pancreas than in the lungs. The expression is seen on the exocrine pancreas as well as on the islets. Exocrine pancreatic injury is manifested as elevated serum amylase and/or lipase in 1–2% and 17% of patients with non-severe and severe COVID-19, respectively . Although any major illness can be associated with stress-related hyperglycemia, studies have reported that patients with SARS (caused by SARS-CoV, the ‘cousin’ of SARS-CoV-2) who had never received glucocorticoids had significantly higher fasting plasma glucose levels as compared to patients with non-SARS pneumonia. In another study, SARS-CoV-mediated damage of the pancreatic β-cells was proposed as the plausible mechanism behind the development of ‘acute diabetes’ in patients with SARS. In fact, immunohistochemistry and in situ hybridization have identified SARS-CoV in the pancreas of patients who died of SARS. Thus, although coronavirus does not feature in the list of viruses implicated in the etiopathogenesis of type 1 diabetes mellitus (T1DM), SARS-CoV (and perhaps SARS-CoV-2) could be potential environmental triggers for the development of T1DM. Apart from direct β-cell damage, alterations in self-antigens and subsequent immune-mediated destruction of β-cells could be implicated. In addition, infection of the surrounding exocrine pancreas by SARS-CoV and SARS-CoV-2 might cause a bystander β-cell death via release of mediators such as tumor-necrosis factor-α (TNFα) and interferon-γ . A systemic pro-inflammatory milieu, as evident by high amounts of interleukin-1β, monocyte chemoattractant protein-1 (MCP-1) and inducible protein-10 even in patients with mild COVID-19 plays an additional role to accentuate the process.
- COVID-19 could also lead to worsening of insulin resistance in patients with pre-existing type 2 diabetes mellitus (T2DM). Apart from inducing a plethora of cytokines, SARS-CoV increases serum levels of fetuin A, a glycoprotein that has been linked with impaired insulin sensitivity. Lopinavir-ritonavir used for the treatment of COVID-19 could lead to lipodystrophy and subsequent insulin resistance. Moreover, COVID-19 is often associated with hypokalemia; this has been attributed to downregulation of pulmonary ACE2, reduced angiotension-II degradation and subsequent increased aldosterone secretion. Hypokalemia, in turn, can worsen glucose control in patients with pre-existing T1DM and T2DM.
- The presence of diabetes mellitus in patients with COVID-19 is associated with severe disease, acute respiratory distress syndrome (ARDS) and increased mortality. Possible explanations include compromised innate immunity and downregulated ACE2 levels in people with diabetes mellitus. In addition, serum levels of inflammation-related biomarkers (interleukin-6, serum ferritin, C-reactive protein) and coagulation parameter (D-dimer) are higher in COVID-19 patients with underlying diabetes mellitus compared with those without, suggesting that people with diabetes are more susceptible to cytokine storm ultimately leading to ARDS and rapid deterioration. Hitherto available studies do not make any distinction between T1DM and T2DM and it is likely that the COVID-19-related risks holds true for both the disease entities . Nevertheless, it is imperative that people with diabetes mellitus (T1DM and T2DM) take extra precautions and stringently implement social distancing and hand hygiene amid this pandemic. In addition, good glycemic control should be ensured. Certain anti-diabetic drugs like pioglitazone (via peroxisome proliferator-activated receptor γ activation) and liraglutide (via glucagon-like peptide 1 receptor activation) have been shown to upregulate ACE2 in animal models ; however, the current evidence does not support any change in the ongoing medications . Similarly, international organizations recommend patients on ACEi/ARBs to carry on with their medications.
- Obesity has also been found to be associated with severe disease in COVID-19. Adipose tissue express ACE2; with higher adipose tissue, more would be the overall ACE2 expression that would act as receptors for SARS-CoV-2. As in diabetes mellitus, even in basal state, obese patients have a higher concentration of several pro-inflammatory cytokines such as TNFα, IL-6 and MCP-1, produced by visceral and subcutaneous adipose tissue. This could again predispose an obese individual to an exaggerated cytokine response in the presence of SARS-CoV-2, manifesting as severe disease and ARDS. In addition, obesity is associated with subclinical hypothyroidism and functional hypogonadism that, at least in part, is mediated by cytokines . These could be aggravated amid a pro-inflammatory milieu induced by COVID-19.
COVID-19 and gonads
- A high level of ACE2 expression is seen in the testes; in fact, the mRNA and protein expression of ACE2 in the testis is almost the highest in the human body. Moreover, the Leydig cells, Sertoli cells and the spermatogonia all express ACE2. Nevertheless, serum testosterone levels in COVID-19 needs to be interpreted cautiously, as any acute critical illness can lead to suppression of the hypothalamic-pituitary-testicular axis, biochemically manifesting as low luteinizing hormone (LH), follicle-stimulating hormone (FSH) and testosterone. However, a recent study in 81 men with COVID-19 showed that serum total testosterone (T) was lower (although not statistically significant), while serum LH was significantly higher as compared to 100 age-matched healthy men. Serum T:LH ratio was also significantly lower in COVID-19 patients and was negatively associated with disease severity. Elevated serum LH in men with COVID-19 negates the possibility of suppression of the hypothalamic-pituitary-testicular axis and hints toward primary Leydig cell damage. In accordance with this observation, it is to be noted that orchitis was indeed a known complication of SARS. In addition, SARS-CoV infection was shown to significantly reduce serum testosterone in male mice. Nevertheless, data on female gonadal function in women with COVID-19 (or SARS) is not available.
COVID-19 and adrenal gland
- One of the primary immunoinvasive strategy utilized by the SARS-CoV, like the influenza virus, is to knock down the host’s cortisol stress response. A very interesting hypothesis that had been proposed is the expression of certain amino acid sequences by the SARS-CoV that are molecular mimics of the host adrenocorticotropic hormone (ACTH). This form of molecular mimicry can indeed blunt the stress-induced cortisol rise, as antibodies produced against the viral particles will inadvertently destroy the circulating ACTH . The fact that most of the SARS-CoV-2 proteins are highly homologous (95–100%) to the proteins of the original SARS-CoV makes us wonder whether SARS-CoV-2 might be employing the same strategy of molecular mimicry as well . Therefore, patients with severe COVID-19 may be more prone to develop critical illness-related corticosteroid insufficiency (CIRCI). Data on cortisol dynamics in patients with COVID-19 are however not yet available. Nevertheless, clinicians must be vigilant about the possibility of an underlying relative cortisol deficiency in patients with COVID-19. Notably, indiscriminate use of short-duration, high-dose glucocorticoids during the SARS outbreak was questioned and not found to be universally useful. One recent study in 31 patients with COVID-19 showed that corticosteroid treatment was not associated with virus clearance time, length of hospital stay or duration of symptoms. Another clinical trial on the efficacy and safety of corticosteroids in COVID-19 is currently underway ( NCT04273321). Nevertheless, patients with underlying primary adrenal insufficiency (PAI) are at a high risk of lower-respiratory tract infections and hence should take extra precautions amid the ongoing pandemic. They should be aware of sick-day guidelines and increase the dose of corticosteroids by themselves whenever suspected of having COVID-19 to avoid an impending adrenal crisis. PAI patients developing COVID-19 may require parenteral glucocorticoid support; serum potassium should be strictly monitored in such patients, as hypokalemia has been reported in patients with COVID-19.
COVID-19 and the hypothalamus-pituitary
- Neurological manifestations do occur in patients with COVID-19 and include, among others, hyposmia. Expression of ACE2 by the olfactory epithelial supporting cells could explain much of these olfactory symptoms . The portal of entry of the virus into the central nervous system (CNS) remains uncertain and could be via hematogenous route or directly thorough the cribriform plate. Hypothalamic and pituitary tissues do express ACE2 and can theoretically be the viral targets. In fact, on autopsy studies, edema and neuronal degeneration along with identification of SARS genome have been shown in the hypothalamus. Biochemical evidence of hypothalamo-pituitary involvement in SARS was first reported by Leow et al. in 2005. Sixty-one survivors of SARS were evaluated at 3 months post-recovery and thereafter periodically. Forty percent of patients had evidence of central hypocortisolism, the majority of which (62.5%) resolved within a year. Of note, 87.5% of those with central hypocortisolism had experienced fatigue and/or postural dizziness at the time of initial recruitment. A small percentage of patients (5%) also had central hypothyroidism. The authors had proposed the possibility of a reversible hypophysitis or a direct hypothalamic damage that could have led to a state of hypothalamo-pituitary dysfunction. Currently, we do not have any such data with regard to patients with COVID-19; however, considering the high frequency of neurological symptoms, one can assume that SARS-CoV-2 may affect the hypothalamus-pituitary as well, directly or via immune-mediated hypophysitis. Accordingly, clinicians should have a low threshold to suspect central hypocortisolism in COVID-19 survivors, especially those complaining of unexplained fatigue, lassitude, malaise, orthostatic dizziness, anorexia and apathy. Patients with pituitary-hypothalamic disorders often have underlying diabetes insipidus (DI); COVID-19 in patients with DI can lead to insensible water loss due to fever and tachypnea ultimately resulting in hypernatremia [ 26]. Hence, the patient and the treating physician need to be cautious in this regard.
COVID-19 and thyroid
- Data on thyroid involvement by coronavirus is most scarce. A study conducted during the SARS outbreak in 2003 had reported that serum T3 and T4 levels were lower in patients with SARS as compared to controls both during the acute and convalescent phases. This could simply imply an underlying sick-euthyroid syndrome. Intensive care patients with sick-euthyroid syndrome tend to have lower mean thyroid weight as a result of reduction in thyroid follicular size associated with depletion of colloid . However, an autopsy study in five patients with SARS has shown marked destruction of the follicular and parafollicular cells of thyroid . Destruction of follicular cells would manifest as low T3 and T4; parafollicular cell damage would theoretically lead to low levels of serum calcitonin. This has been proposed as a plausible mechanism of osteonecrosis of femoral head seen in recovered patients with SARS; calcitonin deficiency leads to disinhibition of osteoclasts leading to osteonecrosis. Data on thyroid function or thyroid pathology are yet not available in COVID-19. The British Thyroid Association and the Society for Endocrinology (BTA/SfE) have issued a consensus statement regarding issues specific to thyroid dysfunction during COVID-19 pandemic. Patients with underlying hypothyroidism or hyperthyroidism are advised to continue their prescribed medications as usual. However, patients on anti-thyroid drugs (ATDs) are at a risk of agranulocytosis, albeit rarely. Symptoms of agranulocytosis often overlap with those of COVID-19, hence, often making it difficult to differentiate one from the other clinically. Hence, it is recommended that patients on ATDs who develop symptoms suggestive of agranulocytosis should immediately discontinue the drug and get a full blood count done at the earliest.
Conclusions
- Amid the ongoing pandemic, endocrine involvement with COVID-19 remains largely unexplored. The aforementioned data pertaining to COVID-19 and the endocrine system are mostly conjectural and factual at this point of time. Validated conclusions must not be drawn based on the presented data, as much of the observations are based on prior experience with SARS and on recent literature derived from small-scale studies. However, the data do provide ample scope for future research. As premature as it may sound, endocrinologists need to be aware of these possibilities in clinical practice, especially while dealing with COVID-19 survivors.
HOW TO USE AYURVEDA TO BALANCE YOUR HORMONES
- In everyday conversations, we often blame things on our hormones, yet most people have only a vague idea of what these actually are. In short, hormones are chemical messengers our bodies produce through the glands in our endocrine system (i.e., thyroid, pancreas, testes, ovaries, etc.). These hormones have powerful effects on many of our bodies’ basic processes, from regulating hunger to influencing our reproductive systems. They affect our moods, our weight, our sleep patterns — you name it.
- Not so incidentally, Ayurveda (a 5,000-year-old holistic health system that originated in India) is concerned with all of these functions of our mind-body as well: Together, they amount to our overall well-being. These messengers form what Ayurveda calls “Dhatu Agni” (or cellular fire), which categorises hormones and enzymes into groups by function, such as digestion or reproduction, rather than chemical classification like in modern medicine. It understands that “the control and functioning of each hormone in our body is regulated by an equal and opposite hormone produced from a completely different anatomical location,” according to Mathew, so unlike modern science, Ayurveda seldom treats the affected gland alone.
- Instead, the Ayurvedic guidelines are concerned with overall balance. With the combined knowledge of Ayurveda and your personal system, you can intuitively learn how to remedy any ills caused by both choices and situations out of your control. To use the wisdom of Ayurveda to bring yourself into balance is not about a diet or a quick-fix solution — which is always the more popular approach in a time-poor, fast-moving world of instant gratification — but a lifestyle overhaul.
- Instead of spot-treating the symptoms that arrive once we already feel ill or out of balance, through Ayurveda we are able to recognise, read, and respond to our symptoms, or signals, from a 360-degree approach. Treating the Dhatu Agni treats the issue by balancing the feedback mechanism, not by introducing more of a particular hormone externally. The effect of various foods and herbs on these functions are the basis of Ayurvedic treatment, not their effect on a particular hormone. Ayurveda offers us effective tools not only to begin to reverse problems, but even more helpfully, to avoid going off balance in any significant way in the first place. Prevention is better than cure.
- Essentially, Ayurveda teaches us that in order to regulate our hormones we need to bring balance into our lives — and that means mind, body, and spirit. We should understand our hormones do not go out of balance in a vacuum. They merely respond to our experiences: our relationships, emotions, reactions, thoughts, and environment. Thought and experience create biology. Hormones will come into balance when our lives come into balance.
- In short, the West seeks to rebalance our hormones externally to promote well-being, but often addressing the symptom is a short-term fix, which may lead to further complications. In the modern world, we are currently experiencing a lot of hormone dependency issues as it leaves less room for our system to learn and rebalance. Introducing a synthetic hormone might be a requirement in certain medical conditions, but it destroys the delicate feedback mechanism that helps the balance of hormones within our body. On the other hand, the Ayurvedic philosophy is a manual on how to assess ourselves holistically, how to look after ourselves properly, and how to troubleshoot if something goes wrong, thereby directly sorting the imbalances that lead to hormonal issues that often arise from leading a life out of balance. Since the effect of the opposing hormones are not ignored in Ayurvedic treatment methods, the body learns from the recovery process.
- So what can we do for ourselves? The first point of call is to rethink our attitude and lifestyle, coming back to nature: following the circadian rhythm of the Earth for restorative sleep, eating, breathing, and moving mindfully, while reducing excessive stimuli and hormone-disrupting blue light during the evenings and getting adequate daylight during the day. Then we need to look at what, how, and when we eat, as this has a huge bearing on our well-being and affects our Agni, or digestive fire. Kindling our digestive fire is perhaps one of the most valuable things you can do to feel at your best. In practice, this also means privileging well-cooked foods made with fresh, local, seasonal, responsibly sourced ingredients and getting familiar with the combinations that can upset your stomach .
- In a less global sense, balancing your hormones is necessarily related to both your natural and your current constitution, that is your Dosha type in its resting state (Prakriti) and your Dosha type in your environment and individual circumstances (Vikriti). Your Dosha type is your Ayurvedic mind-body type, which can be described through three Doshas: Vata (air), Pitta (fire), and Kapha (earth). Each Dosha has a set of characteristics, and each person is made up of a unique combination of all three, typically with one dominant one. Feeling in balance is more of an awareness of the dominant Doshas or your unique body type, and considering this uniqueness when making diet and lifestyle choices. For example, if you’re feeling stressed, stretched thin by the demands of your big city life, which are flighty vata characteristics, you should choose grounding foods and practices, like eating a warm bowl of soup or meditating. It is a very intuitive system; it just takes a bit of familiarisation.
- If you feel an imbalance in a certain area of your life, the next thing to do is to look into remedies you can introduce at home and observe how they make you feel. Adaptogens, an Ayurvedic remedy, are gaining traction in the West as a way to balance our hormones by adapting to your body and its needs and can help get us through a sticky patch while we get our lives in order. The important thing to note here again is that this isn’t the fix-all that we may want it to be, because holistic medicine is not a one-size-fits-all approach, but more a means of understanding yourself as complex, ever-changing, and one with the world. Start by researching adaptogens that might help you with something specific you’re experiencing. You could try shatavari tea for balancing pitta or supporting your reproductive system (including periods or menopause) or amla powder for a vitamin C boost or if you’re feeling dehydrated.
- Finally, although it’s OK to take adaptogens in small doses of your own accord, it is always better to work with an Ayurvedic doctor for specific tinctures and more potent herbal remedies. And if you’re feeling particularly out of whack, it may be time to consider a Panchakarma (Ayurvedic detox) in conjunction with a Vaidya (practitioner). This is a faster route to unraveling the actions that have brought us out of balance than just integrating Ayurveda slowly.
Chakras and Endocrine system


- The word chakra comes from the Sanskrit meaning “wheel” or “disk”.The origins of the sevenfold Chakra system is said to come from the Vedas, the four holy books of the Hindus believed to date back before 2500 B.C. Chakra symbols are traditionally depicted as lotus flowers, each resonating at different frequencies, corresponding to the colors of the rainbow. Hindu system names seven major chakras, meanwhile the human energy system is said to have many chakras, and new ones are being discovered every day. Each chakra is positioned through the spinal column, or Sushumna, from the coccyx to the crown of the head. Imbalance in one chakra affects the others, same as nervous and endocrine systems are functionally interconnected and any disturbance in one part can lead to the problem elsewhere. The endocrine system acts as a great network of communication between brain and body and is responsible for various metabolic functions that facilitate cellular communication as well as stimulation and hormone release. For the entire human body to function well these endocrine glands must produce and maintain a balance of these various fluids and hormones. To understand how the endocrine system is connected with chakras, let us see each pair in order.


Adrenals — Root Chakra
- The adrenals are triangular-shaped glands that cap each of the kidneys. They produce a variety of hormones which regulate the body`s metabolism and ones that control the balance of salt and body fluids. These glands also produce adrenalin, the hormone essential with our primitive “fight or flight” response, from with we can determine the link between this gland and the Root chakra`s association with the physical survival.


Ovaries/Testes — Sacral Chakra
- The male and female reproductive organs, produce hormones that regulate individual sexual development, amount of the body hair, depth of the voice and production of sperm and eggs in females. The key associated with this chakra is the relationship with our sexuality and emotional balance.


Pancreas — Solar Plexus Chakra
- The pancreas located behind the stomach and secretes different substances for effective digestion. It also produces insulin which helps to control sugar in the blood. One of the physical dysfunction of this chakra is diabetes. There is a further link with the Solar Plexus Chakra and adrenalin, which is why we experience “butterflies in the stomach” during exciting moments in our life. The key association — digestive system, further dysfunction of this chakra is stomach ulcers.


Thymus — Heart Chakra
- The thymus — located just above the chest, produces hormones that stimulate general growth, in infancy. Interesting that infants have much larger thymus size than adults. Thymus provides strong immunity system by stimulating the production of lymphocytes, which the part of the body`s defense system. Nowadays, scientists recognize that auto-immune diseases, where the immune system attacks its proteins, mistaking them for a foreign substance, have an emotional connection and are not simply because of physical or environmental causes.


Thyroid | Parathyroid — Throat Chakra
- The thyroid the gland is located behind trachea in the neck, produces thyroxine, it plays a major role in the metabolism, growth, and development of the human body. It helps to regulate many body functions by constantly releasing a steady amount of thyroid hormones into the bloodstream. Parathyroid glands regulate calcium levels in the bloodstream. The throat chakra is linked with all forms of communication, corresponds to the need for the balance between the rational, cerebral approach and the emotional expression of the heart.


Pituitary — Third eye Chakra
- The pituitary bland is called the master of gland because it`s involved in so many processes. Its is located within a structure at the base of the skull, near the underside of the brain. It`s also attached the hypothalamus. This vital gland influences growth, metabolism, endorphins ( pain-relieving properties ), prolactin (helps women who are breastfeeding to produce milk), stimulates adrenal glands. Also, this includes estrogen which produces contractions during labor and also helps to release milk from the breasts. It is interesting that the Third eye-pituitary gland connection with birth and motherhood, a time when many women feel that their intuition, particularly about their child, is at its peak.


Pineal — Crown Chakra
- The pineal gland — is a small, pea-shaped gland in the brain. Still has mystical properties. But we do now that it produces melatonin which is responsible to regulate our sleep patterns, anti-aging properties and is believed to affect the pituitary, thyroid, adrenals, and gonads — although no one yet understands exactly how. As the Crown`s function within the chakra system as a whole, the pineal gland is the control center for the effective functioning of our physical, emotional and mental selves.
In the same way that our physical body`s central nervous system consists of the spinal cord leading o the brain, the energetic equivalent is “Sushumna” — the vertical column through which all chakras are located. Sushumna is the primary of the three main nadis ( channels of energy ) in the body. While the Sushumna is the central channel, the “ida” left and “Pingala” right nadis start and end on opposite sides of Sushumna. In yoga and health science of Ayurveda, it is thought that keeping nadis in balance and free from blocks promotes the flow of prana ( vital energy ), which increases physical and mental health. The principal ways of balancing the nadis in yoga practice are through pranayama ( breathing exercises ) and meditation.
Ways To Reset Your Hormones For Health, Energy & Weight Control
When you focus on fixing the underlying dysfunctions, your hormones will find that nice, healthy balance, no matter what your age. So here’s where to start:
Cut back — way back — on the sweets and starches.
- Too many can set your hormones on a wild ride. Even better: eliminate sweets and starches altogether for two weeks to see how your body reacts.
Try reducing your grains, legumes and high sugar fruits for two weeks.
- You may unknowingly be carbohydrate-intolerant. Over-doing it on these carbs can cause metabolic problems for those of us who are insulin-resistant or who don’t process carbohydrates efficiently.
Eat more healthy fats. (And let go of fat-phobia.)
- Too few good fats on your plate will short-change your body’s ability to produce the hormones that boost energy, feelings of satiety and suppress cravings.
Be good to your microbiome.
- In other words: feed your gut with plenty of immunity-supporting fermented foods and belly-benefiting fiber to support good bacteria and keep bad bacteria in check. This will not only keep digestion and elimination running smoothly, but help hormone function too.
Avoid reactive, inflammatory foods.
- For starters, stay away from sugar, gluten, processed foods and junk food, as they over-tax your immune system, gut and endocrine system.
Aim to sleep more and better.
- Not enough sleep or poor quality sleep wreaks havoc on your system, limiting your body’s ability to release the hormones necessary to repair, restore and refresh cells as you snooze. The result? A more rapidly aging body and brain. (No thanks!) Shoot for 7 to 8 hours a night to enable your hormones to do their job.
Cool it on the stimulants.
- Too much caffeine in the form of coffee, energy drinks, sodas, and sometimes even tea or chocolate interfere with the hormones that promote restorative sleep.
Cut the chemicals.
- There’s no hormonal upside to ongoing low-level exposure to common chemicals in your food, air, water, household cleaners, personal-care products and cosmetics. In fact, they interfere with optimal hormonal function. Make an effort to switch to the least toxic, most natural products possible to limit exposure to chemicals .
Minimize the meds.
- Ongoing exposure to meds, including both over-the-counter remedies and prescription drugs, can stress our microbiomes and throw hormones out of whack. Avoid hormone-disrupting OTC meds and, if you must take prescription drugs, ask the doc to prescribe the smallest therapeutic dose possible.
Train yourself to unwind in ways that enhance healthy hormone function.
- Whether you’re dealing with unremitting life challenges or bouts of intermittent stress, remember to blow off steam regularly: find a funny movie and laugh uproariously, put on some music and “dance it out,” or treat yourself to a night out and have some well-deserved fun! Add to that a regular meditation and a simple, restorative yoga practice and you’ll be well on your way to balancing your hormones, in addition to staying more relaxed, fit and trim.
The Endocrine System : An Overview
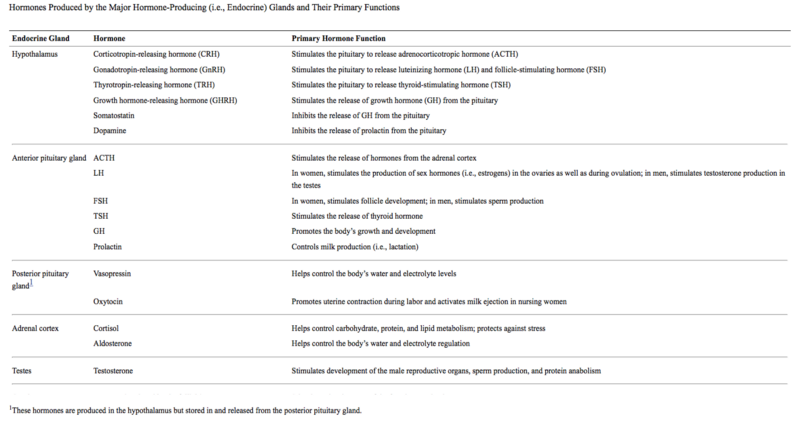
- A plethora of hormones regulate many of the body’s functions, including growth and development, metabolism, electrolyte balances, and reproduction. Numerous glands throughout the body produce hormones. The hypothalamus produces several releasing and inhibiting hormones that act on the pituitary gland, stimulating the release of pituitary hormones. Of the pituitary hormones, several act on other glands located in various regions of the body, whereas other pituitary hormones directly affect their target organs. Other hormone-producing glands throughout the body include the adrenal glands, which primarily produce cortisol; the gonads (i.e., ovaries and testes), which produce sex hormones; the thyroid, which produces thyroid hormone; the parathyroid, which produces parathyroid hormone; and the pancreas, which produces insulin and glucagon. Many of these hormones are part of regulatory hormonal cascades involving a hypothalamic hormone, one or more pituitary hormones, and one or more target gland hormones.
- For the body to function properly, its various parts and organs must communicate with each other to ensure that a constant internal environment (i.e., homeostasis) is maintained. For example, neither the body temperature nor the levels of salts and minerals (i.e., electrolytes) in the blood must fluctuate beyond preset limits. Communication among various regions of the body also is essential for enabling the organism to respond appropriately to any changes in the internal and external environments. Two systems help ensure communication: the nervous system and the hormonal (i.e., neuroendocrine) system. The nervous system generally allows rapid transmission (i.e., within fractions of seconds) of information between different body regions. Conversely, hormonal communication, which relies on the production and release of hormones from various glands and on the transport of those hormones via the bloodstream, is better suited for situations that require more widespread and longer lasting regulatory actions. Thus, the two communication systems complement each other. In addition, both systems interact: Stimuli from the nervous system can influence the release of certain hormones and vice versa.
- Generally speaking, hormones control the growth, development, and metabolism of the body; the electrolyte composition of bodily fluids; and reproduction. Here we provide an overview of the hormone systems involved in those regulatory processes. We first summarize some of the basic characteristics of hormone-mediated communication within the body, then review the various glands involved in those processes and the major hormones they produce. We presents various endocrine systems in which hormones produced in several organs cooperate to achieve the desired regulatory effects. The discussions focus primarily on the system responses in normal, healthy people. We discuss how endocrine system impacts immunity. Finally we share thoughts how the health of the endocrine system is very important for not surviving but thriving.
What Are Hormones?
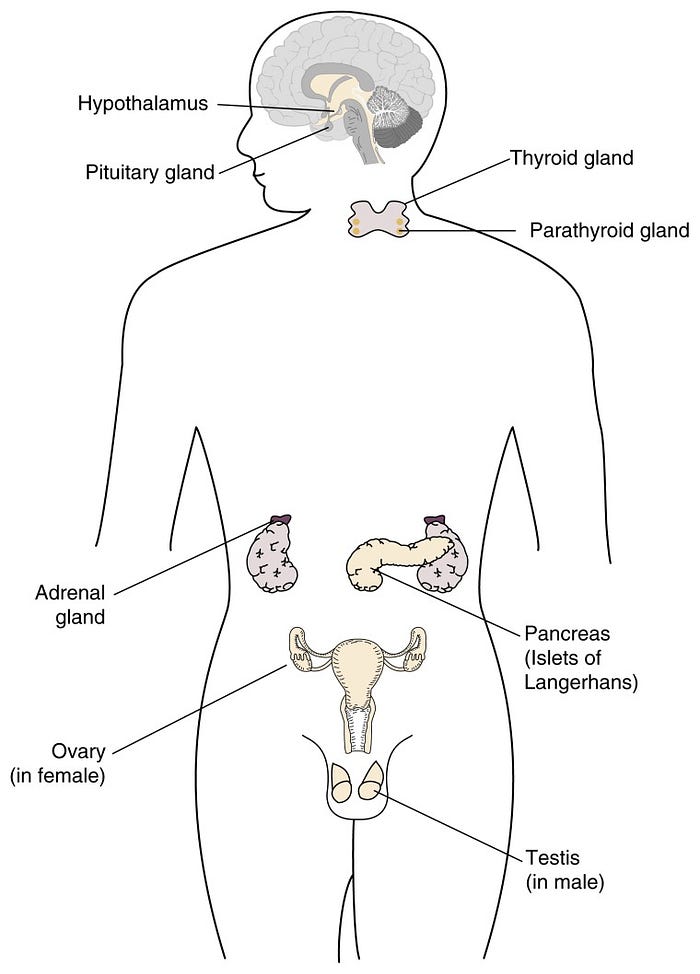
- Hormones are molecules that are produced by endocrine glands, including the hypothalamus, pituitary gland, adrenal glands, gonads, (i.e., testes and ovaries), thyroid gland, parathyroid glands, and pancreas (figure 1). The term “endocrine” implies that in response to specific stimuli, the products of those glands are released into the bloodstream. The hormones then are carried via the blood to their target cells. Some hormones have only a few specific target cells, whereas other hormones affect numerous cell types throughout the body. The target cells for each hormone are characterized by the presence of certain docking molecules (i.e., receptors) for the hormone that are located either on the cell surface or inside the cell. The interaction between the hormone and its receptor triggers a cascade of biochemical reactions in the target cell that eventually modify the cell’s function or activity.

Mechanisms of Action
- Several classes of hormones exist, including steroids, amino acid derivatives, and polypeptides and proteins. Those hormone classes differ in their general molecular structures (e.g., size and chemical properties). As a result of the structural differences, their mechanisms of action (e.g., whether they can enter their target cells and how they modulate the activity of those cells) also differ. Steroids, which are produced by the gonads and part of the adrenal gland (i.e., the adrenal cortex), have a molecular structure similar to that of cholesterol. The molecules can enter their target cells and interact with receptors in the fluid that fills the cell (i.e., the cytoplasm) or in the cell nucleus. The hormone-receptor complexes then bind to certain regions of the cell’s genetic material (i.e., the DNA), thereby regulating the activity of specific hormone-responsive genes.
- Amino acid derivatives are modified versions of some of the building blocks of proteins. The thyroid gland and another region of the adrenal glands (i.e., the adrenal medulla) produce this type of hormone (i.e., the amino acid derivatives). Like steroids, amino acid derivatives can enter the cell, where they interact with receptor proteins that are already associated with specific DNA regions. The interaction modifies the activity of the affected genes.
- Polypeptide and protein hormones are chains of amino acids of various lengths (from three to several hundred amino acids). These hormones are found primarily in the hypothalamus, pituitary gland, and pancreas. In some instances, they are derived from inactive precursors, or pro-hormones, which can be cleaved into one or more active hormones. Because of their chemical structure, the polypeptide and protein hormones cannot enter cells. Instead, they interact with receptors on the cell surface. The interaction initiates biochemical changes in either the cell’s membrane or interior, eventually modifying the cell’s activity or function.
Regulation of Hormone Activity
- To maintain the body’s homeostasis and respond appropriately to changes in the environment, hormone production and secretion must be tightly controlled. To achieve this control, many bodily functions are regulated not by a single hormone but by several hormones that regulate each other (see ). For example, for many hormone systems, the hypothalamus secretes so-called releasing hormones, which are transported via the blood to the pituitary gland. There, the releasing hormones induce the production and secretion of pituitary hormones, which in turn are transported by the blood to their target glands (e.g., the adrenal glands, gonads, or thyroid). In those glands, the interaction of the pituitary hormones with their respective target cells results in the release of the hormones that ultimately influence the organs targeted by the hormone cascade.

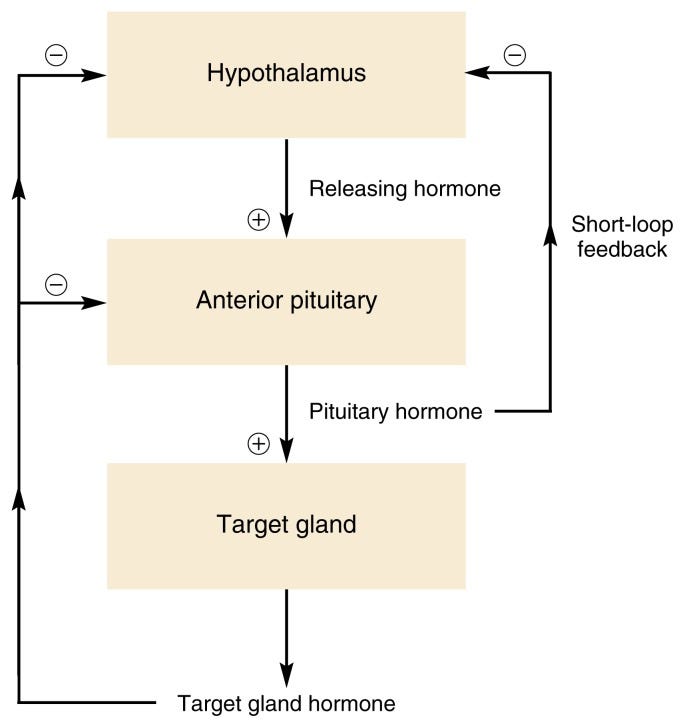
- Constant feedback from the target glands to the hypothalamus and pituitary gland ensures that the activity of the hormone system involved remains within appropriate boundaries. Thus, in most cases, negative feedback mechanisms exist by which hormones released by the target glands affect the pituitary gland and/or hypothalamus (figure 2 ). When certain predetermined blood levels of those hormones are reached, the hypothalamus and/or the pituitary ceases hormone release, thereby turning off the cascade. In some instances, a so-called short-loop feedback occurs, in which pituitary hormones directly act back on the hypothalamus.
- The sensitivity with which these negative feedback systems operate (i.e., the target hormone levels that are required to turn off hypothalamic or pituitary hormone release) can change at different physiological states or stages of life. For example, the progressive reduction in sensitivity of the hypothalamus and pituitary to negative feedback by gonadal steroid hormones plays an important role in sexual maturation.
- Although negative feedback is more common, some hormone systems are controlled by positive feedback mechanisms, in which a target gland hormone acts back on the hypothalamus and/or pituitary to increase the release of hormones that stimulate the secretion of the target gland hormone. One such mechanism occurs during a woman’s menstrual period: Increasing estrogen levels in the blood temporarily stimulate, rather than inhibit, hormone release from the pituitary and hypothalamus, thereby further increasing estrogen levels and eventually leading to ovulation. Such a mechanism requires a specific threshold level, however, at which the positive feedback loop is turned off in order to maintain a stable system.
The Hypothalamus and Its Hormones
- The hypothalamus is a small region located within the brain that controls many bodily functions, including eating and drinking, sexual functions and behaviors, blood pressure and heart rate, body temperature maintenance, the sleep-wake cycle, and emotional states (e.g., fear, pain, anger, and pleasure). Hypothalamic hormones play pivotal roles in the regulation of many of those functions.
- Because the hypothalamus is part of the central nervous system, the hypothalamic hormones actually are produced by nerve cells (i.e., neurons). In addition, because signals from other neurons can modulate the release of hypothalamic hormones, the hypothalamus serves as the major link between the nervous and endocrine systems. For example, the hypothalamus receives information from higher brain centers that respond to various environmental signals. Consequently, hypothalamic function is influenced by both the external and internal environments as well as by hormone feedback. Stimuli from the external environment that indirectly influence hypothalamic function include the light-dark cycle; temperature; signals from other members of the same species; and a wide variety of visual, auditory, olfactory, and sensory stimuli. The communication between other brain areas and the hypothalamus, which conveys information about the internal environment, involves electrochemical signal transmission through molecules called neurotransmitters (e.g., aspartate, dopamine, gamma-aminobutyric acid, glutamate, norepinephrine, and serotonin). The complex interplay of the actions of various neurotransmitters regulates the production and release of hormones from the hypothalamus.
The hypothalamic hormones are released into blood vessels that connect the hypothalamus and the pituitary gland (i.e., the hypothalamic-hypophyseal portal system). Because they generally promote or inhibit the release of hormones from the pituitary gland, hypothalamic hormones are commonly called releasing or inhibiting hormones. The major releasing and inhibiting hormones include the following :
- Corticotropin-releasing hormone (CRH), which is part of the hormone system regulating carbohydrate, protein, and fat metabolism as well as sodium and water balance in the body
- Gonadotropin-releasing hormone (GnRH), which helps control sexual and reproductive functions, including pregnancy and lactation (i.e., milk production)
- Thyrotropin-releasing hormone (TRH), which is part of the hormone system controlling the metabolic processes of all cells and which contributes to the hormonal regulation of lactation
- Growth hormone-releasing hormone (GHRH), which is an essential component of the system promoting the organism’s growth
- Somatostatin, which also affects bone and muscle growth but has the opposite effect as that of GHRH
- Dopamine, a substance that functions primarily as a neurotransmitter but also has some hormonal effects, such as repressing lactation until it is needed after childbirth.
The Pituitary and Its Major Hormones
- The pituitary (also sometimes called the hypophysis) is a gland about the size of a small marble and is located in the brain directly below the hypothalamus. The pituitary gland consists of two parts: the anterior pituitary and the posterior pituitary.
The Anterior Pituitary
- The anterior pituitary produces several important hormones that either stimulate target glands (e.g., the adrenal glands, gonads, or thyroid gland) to produce target gland hormones or directly affect target organs. The pituitary hormones include adrenocorticotropic hormone (ACTH); gonadotropins; thyroid-stimulating hormone (TSH), also called thyrotropin; growth hormone (GH); and prolactin.
- The first three of those hormones-ACTH, gonadotropins, and TSH-act on other glands. Thus, ACTH stimulates the adrenal cortex to produce corticosteroid hormones-primarily cortisol-as well as small amounts of female and male sex hormones. The gonadotropins comprise two molecules, luteinizing hormone (LH) and follicle-stimulating hormone (FSH). These two hormones regulate the production of female and male sex hormones in the ovaries and testes as well as the production of the germ cells-that is, the egg cells (i.e., ova) and sperm cells (i.e., spermatozoa). TSH stimulates the thyroid gland to produce and release thyroid hormone. The remaining two pituitary hormones, GH and prolactin, directly affect their target organs.
Growth Hormone
- GH is the most abundant of the pituitary hormones. As the name implies, it plays a pivotal role in controlling the body’s growth and development. For example, it stimulates the linear growth of the bones; promotes the growth of internal organs, fat (i.e., adipose) tissue, connective tissue, endocrine glands, and muscle; and controls the development of the reproductive organs. Accordingly, the GH levels in the blood are highest during early childhood and puberty and decline thereafter. Nevertheless, even relatively low GH levels still may be important later in life, and GH deficiency may contribute to some symptoms of aging.
- In addition to its growth-promoting role, GH affects carbohydrate, protein, and fat (i.e., lipid) metabolism. Thus, GH increases the levels of the sugar glucose in the blood by reducing glucose uptake by muscle cells and adipose tissue and by promoting glucose production (i.e., gluconeogenesis) from precursor molecules in the liver. GH also enhances the uptake of amino acids from the blood into cells, as well as their incorporation into proteins, and stimulates the breakdown of lipids in adipose tissue.
- To elicit these various effects, GH modulates the activities of numerous target organs, including the liver, kidneys, bone, cartilage, skeletal muscle, and adipose cells. For some of these effects, GH acts directly on the target cells. In other cases, however, GH acts indirectly by stimulating the production of a molecule called insulin-like growth factor 1 (IGF-1) in the liver and kidneys. The blood then transports IGF-1 to the target organs, where it binds to specific receptors on the cells. This interaction then may lead to the increased DNA production and cell division that underlie the growth process.
- Two hypothalamic hormones control GH release: (1) GHRH, which stimulates GH release, and (2) somatostatin, which inhibits GH release. This regulatory mechanism also involves a short-loop feedback component, by which GH acts on the hypothalamus to stimulate somatostatin release. In addition, GH release is enhanced by stress, such as low blood sugar levels (i.e., hypoglycemia) or severe exercise, and by the onset of deep sleep.
- Acute and chronic alcohol consumption have been shown to reduce the levels of GH and IGF-1 in the blood. Both effects have been observed in animals as well as in humans. Acute alcohol administration also reduces GH secretion in response to other stimuli that normally enhance the hormone’s release. Those deleterious effects of alcohol may be particularly harmful to adolescents, who require GH for normal development and puberty.
Prolactin
- Together with other hormones, prolactin plays a central role in the development of the female breast and in the initiation and maintenance of lactation after childbirth. Prolactin’s function in men, however, is not well understood, although excessive prolactin release can lead to reduced sex drive (i.e., libido) and impotence. Several factors control prolactin release from the anterior pituitary. For example, prolactin is released in increasing amounts in response to the rise in estrogen levels in the blood that occurs during pregnancy. In nursing women, prolactin is released in response to suckling by the infant. Several releasing and inhibitory factors from the hypothalamus also control prolactin release. The most important of those factors is dopamine, which has an inhibitory effect.
- Alcohol consumption by nursing women can influence lactation both through its effects on the release of prolactin and oxytocin (see the following section) and through its effects on the milk-producing (i.e., mammary) glands and the composition of the milk.
The Posterior Pituitary
- The posterior pituitary does not produce its own hormones; instead, it stores two hormones-vasopressin and oxytocin-that are produced by neurons in the hypothalamus. Both hormones collect at the ends of the neurons, which are located in the hypothalamus and extend to the posterior pituitary.
- Vasopressin, also called arginine vasopressin (AVP), plays an important role in the body’s water and electrolyte economy. Thus, AVP release promotes the reabsorption of water from the urine in the kidneys. Through this mechanism, the body reduces urine volume and conserves water. AVP release from the pituitary is controlled by the concentration of sodium in the blood as well as by blood volume and blood pressure. For example, high blood pressure or increased blood volume results in the inhibition of AVP release. Consequently, more water is released with the urine, and both blood pressure and blood volume are reduced. Alcohol also has been shown to inhibit AVP release. Conversely, certain other drugs (e.g., nicotine and morphine) increase AVP release, as do severe pain, fear, nausea, and general anesthesia, thereby resulting in lower urine production and water retention.
- Oxytocin, the second hormone stored in the posterior pituitary, stimulates the contractions of the uterus during childbirth. In nursing women, the hormone activates milk ejection in response to suckling by the infant (i.e., the so-called let-down reflex).
The Adrenal Glands and Their Hormones
- The adrenal glands are small structures located on top of the kidneys. Structurally, they consist of an outer layer (i.e., the cortex) and an inner layer (i.e., the medulla). The adrenal cortex produces numerous hormones, primarily corticosteroids (i.e., glucocorticoids and mineralocorticoids). The cortex is also the source of small amounts of sex hormones; those amounts, however, are insignificant compared with the amounts normally produced by the ovaries and testes. The adrenal medulla generates two substances-adrenaline and noradrenaline-that are released as part of the fight-or-flight response to various stress factors.
- The primary glucocorticoid in humans is cortisol (also called hydro-cortisone), which helps control carbohydrate, protein, and lipid metabolism. For example, cortisol increases glucose levels in the blood by stimulating gluconeogenesis in the liver and promotes the formation of glycogen (i.e., a molecule that serves as the storage form of glucose) in the liver. Cortisol also reduces glucose uptake into muscle and adipose tissue, thereby opposing the effects of insulin. Furthermore, in various tissues, cortisol promotes protein and lipid breakdown into products (i.e., amino acids and glycerol, respectively) that can be used for gluconeogenesis.
- In addition to those metabolic activities, cortisol appears to protect the body against the deleterious effects of various stress factors, including acute trauma, major surgery, severe infections, pain, blood loss, hypoglycemia, and emotional stress. All of these stress factors lead to drastic increases in the cortisol levels in the blood. For people in whom cortisol levels cannot increase (e.g., because they had their adrenal glands removed), even mild stress can be fatal. Finally, high doses of cortisol and other corticosteroids can be used medically to suppress tissue inflammation in response to injuries and to reduce the immune response to foreign molecules.
- The primary mineralocorticoid in humans is aldosterone, which also helps regulate the body’s water and electrolyte balance. Its principal functions are to conserve sodium and to excrete potassium from the body. For example, aldosterone promotes the reabsorption of sodium in the kidney, thereby reducing water excretion and increasing blood volume. Similarly, aldosterone decreases the ratio of sodium to potassium concentrations in sweat and saliva, thereby preventing sodium loss via those routes. The effect can be highly beneficial in hot climates, where much sweating occurs.
- In contrast to the glucocorticoids, pituitary, or hypothalamic, hormones do not regulate aldosterone release. Instead, it is controlled primarily by another hormone system, the reninangiotensin system, which also controls kidney function. In addition, the levels of sodium and potassium in the blood influence aldosterone levels.
The Gonads and Their Hormones
- The gonads (i.e., the ovaries and testes) serve two major functions. First, they produce the germ cells (i.e., ova in the ovaries and spermatozoa in the testes). Second, the gonads synthesize steroid sex hormones that are necessary for the development and function of both female and male reproductive organs and secondary sex characteristics (e.g., the adult distribution of body hair, such as facial hair in men) as well as for pregnancy, childbirth, and lactation. Three types of sex hormones exist; each with different functions: (1) estrogens (e.g., estradiol), which exert feminizing effects; (2) progestogens (e.g., progesterone), which affect the uterus in preparation for and during pregnancy; and (3) androgens (e.g., testosterone), which exert masculinizing effects. In addition to the reproductive functions, sex hormones play numerous essential roles throughout the body. For example, they affect the metabolism of carbohydrates and lipids, the cardiovascular system, and bone growth and development.
Estrogens
- The major estrogen is estradiol, which, in addition to small amounts of estrone and estriol, is produced primarily in the ovaries. Other production sites of estrogens include the corpus luteum, the placenta, and the adrenal glands. In men and postmenopausal women, most estrogens present in the circulation are derived from the conversion of testicular, adrenal, and ovarian androgens. The conversion occurs in peripheral tissues, primarily adipose tissue and skin.
- The main role of estrogens is to coordinate the normal development and functioning of the female genitalia and breasts. During puberty, estrogens promote the growth of the uterus, breasts, and vagina; determine the pattern of fat deposition and distribution in the body that results in the typical female shape; regulate the pubertal growth spurt and cessation of growth at adult height; and control the development of secondary sexual characteristics. In adult women, the primary functions of estrogens include regulating the menstrual cycle, contributing to the hormonal regulation of pregnancy and lactation, and maintaining female libido.
- During menopause, estrogen production in the ovaries ceases. The resulting reduction in estrogen levels leads to symptoms such as hot flashes, sweating, pounding of the heart (i.e., palpitations), increased irritability, anxiety, depression, and brittle bones (i.e., osteoporosis). The administration of estrogens (i.e., hormone replacement therapy) can alleviate those symptoms and reduce the risk of osteoporosis and coronary heart disease in postmenopausal women. At the same time, however, hormone replacement therapy may increase the risk of certain types of cancer (e.g., breast cancer and uterine [i.e., endometrial] cancer). Alcohol consumption has been shown to increase estrogen levels in the blood and urine, even in premenopausal women who drink two drinks or less per day and in postmenopausal women who drink less than one drink per day. These findings suggest that moderate alcohol consumption may help prevent osteoporosis and coronary heart disease in postmenopausal women. Other studies, however, have detected no consistent association between alchol consumption and increased estrogen levels .
Progestogens
- The ovaries produce progestogens during a certain phase of the menstrual cycle and in the placenta for most of pregnancy. Progestogens cause changes in the uterine lining in preparation for pregnancy and-together with estrogens-stimulate the development of the mammary glands in the breasts in preparation for lactation. The primary progestogen is progesterone.
Androgens
- The principal androgenic steroid is testosterone, which is secreted primarily from the testes but also, in small amounts, from the adrenal glands (both in men and women) and from the ovaries. Its main function is to stimulate the development and growth of the male genital tract. In addition, testosterone has strong protein anabolic activities-that is, it promotes protein generation, which leads to increased muscle mass. The specific functions of testosterone vary during different developmental stages, as follows:
- In the fetus, testosterone primarily ensures the development of the internal and external male genitalia
- During puberty, testosterone promotes the growth of the male sex organs and is responsible for other male developmental characteristics, such as the pubertal growth spurt and eventual cessation of growth at adult height; deepening of the voice; growth of facial, pubic, axillary, and body hair; and increase in muscularity and strength
- In the adult male, testosterone primarily serves to maintain masculinity, libido, and sexual potency as well as regulate sperm production. Testosterone levels decline slightly with age, although the drop is not as drastic as the reduction in estrogen levels in women during menopause.
The Thyroid and Its Hormones
- The thyroid gland, which consists of two lobes, is located in front of the windpipe (i.e., trachea), just below the voice box (i.e., larynx). The gland produces two structurally related hormones, thyroxine (T 4) and triiodothyronine (T 3), that are iodinated derivatives of the amino acid tyrosine. Both hormones are collectively referred to as “thyroid hormone.” T 4 constitutes approximately 90 percent of the hormone produced in the thyroid gland. However, T 3 is a much more active hormone, and most of the T 4 produced by the thyroid is converted into T 3 in the liver and kidneys.
- Thyroid hormone in general serves to increase the metabolism of almost all body tissues. For example, thyroid hormone stimulates the production of certain proteins involved in heat generation in the body, a function that is essential for maintaining body temperature in cold climates. Moreover, thyroid hormone promotes several other metabolic processes involving carbohydrates, proteins, and lipids that help generate the energy required for the body’s functions. In addition to those metabolic effects, thyroid hormone plays an essential role in the development of the central nervous system during late fetal and early postnatal developmental stages. Furthermore, thyroid hormone exerts an effect similar to that of GH on normal bone growth and maturation. Finally, thyroid hormone is required for the normal development of teeth, skin, and hair follicles as well as for the functioning of the nervous, cardiovascular, and gastrointestinal systems.
- In addition to thyroid hormone, certain cells (i.e., parafollicular C cells) in the thyroid gland produce calcitonin, a hormone that helps maintain normal calcium levels in the blood. Specifically, calcitonin lowers calcium levels in the blood by reducing the release of calcium from the bones; inhibiting the constant erosion of bones (i.e., bone resorption), which also releases calcium; and inhibiting the reabsorption of calcium in the kidneys. Those effects are opposite to those of parathyroid hormone (PTH), which is discussed in the following section.
The Parathyroid Glands and Their Hormones
- The parathyroid glands are four pea-sized bodies located behind the thyroid gland that produce PTH. This hormone increases calcium levels in the blood, helping to maintain bone quality and an adequate supply of calcium, which is needed for numerous functions throughout the body (e.g., muscle movement and signal transmission within cells). Specifically, PTH causes reabsorption of calcium from and excretion of phosphate in the urine. PTH also promotes the release of stored calcium from the bones as well as bone resorption, both of which increase calcium levels in the blood. Finally, PTH stimulates the absorption of calcium from the food in the gastrointestinal tract. Consistent with PTH’s central role in calcium metabolism, the release of this hormone is not controlled by pituitary hormones but by the calcium levels in the blood. Thus, low calcium levels stimulate PTH release, whereas high calcium levels suppress it.
- Many of the functions of PTH require or are facilitated by a substance called 1,25-dihydroxycholecalciferol, a derivative of vitamin D. In addition, numerous other hormones are involved in regulating the body’s calcium levels and bone metabolism, including estrogens, glucocorticoids, and growth hormone.
The Pancreas and Its Hormones
- The pancreas is located in the abdomen, behind the stomach, and serves two distinctly different functions. First, it acts as an exocrine organ, because the majority of pancreatic cells produce various digestive enzymes that are secreted into the gut and which are essential for the effective digestion of food. Second, the pancreas serves as an endocrine organ, because certain cell clusters (i.e., the Islets of Langerhans) produce two hormones-insulin and glucagon-that are released into the blood and play pivotal roles in blood glucose regulation.
Insulin
- Insulin is produced in the beta cells of the Islets of Langerhans. Its primary purpose is to lower blood glucose levels; in fact, insulin is the only blood sugar-lowering hormone in the body. To this end, insulin promotes the formation of storage forms of energy (e.g., glycogen, proteins, and lipids) and suppresses the breakdown of those stored nutrients. Accordingly, the target organs of insulin are primarily those that are specialized for energy storage, such as the liver, muscles, and adipose tissue. Specifically, insulin has the following metabolic effects:
- Promotes glucose uptake into cells and its conversion into glycogen, stimulates the breakdown of glucose, and inhibits gluconeogenesis
- Stimulates the transport of amino acids into cells and protein synthesis in muscle cells, thereby lowering the levels of amino acids available for gluconeogenesis in the liver
- Increases fat synthesis in the liver and adipose tissue, thereby lowering the levels of glycerol, which also can serve as a starting material for gluconeogenesis.
The release of insulin is controlled by various factors, including blood glucose levels; other islet hormones (e.g., glucagon); and, indirectly, other hormones that alter blood glucose levels (e.g., GH, glucocorticoids, and thyroid hormone).
Glucagon
- The second blood-sugar-regulating pancreatic hormone is glucagon, which is produced in the alpha cells of the Islets of Langerhans. Glucagon increases blood glucose levels; accordingly, its main actions generally are opposite to those of insulin. For example, glucagon increases glycogen breakdown and gluconeogenesis in the liver as well as the breakdown of lipids and proteins. The release of glucagon is regulated by many of the same factors as is insulin’s release, but sometimes with the opposite effect. Thus, an increase in blood glucose levels stimulates insulin release but inhibits glucagon release.
- A finely tuned balance between the activities of insulin and glucagon is essential for maintaining blood sugar levels. Accordingly, disturbances of that balance, such as an insulin deficiency or an inability of the body to respond adequately to insulin, result in serious disorders, such as diabetes mellitus.
Hormone Systems
- As this review has indicated in describing the various endocrine glands and their hormones, some hormones are controlled directly by the metabolic pathways that they influence. For example, blood sugar levels directly control insulin and glucagon release by the pancreas, and calcium levels in the blood regulate PTH release. Conversely, many hormones produced by target glands are regulated by pituitary hormones, which in turn are controlled by hypothalamic hormones. Examples of such regulatory hormonal cascades include the hypothalamic-pituitary-adrenal (HPA) axis, the hypothalamic-pituitary-gonadal (HPG) axis, and the hypothalamic-pituitary-thyroidal (HPT) axis, which are described briefly in the following sections.

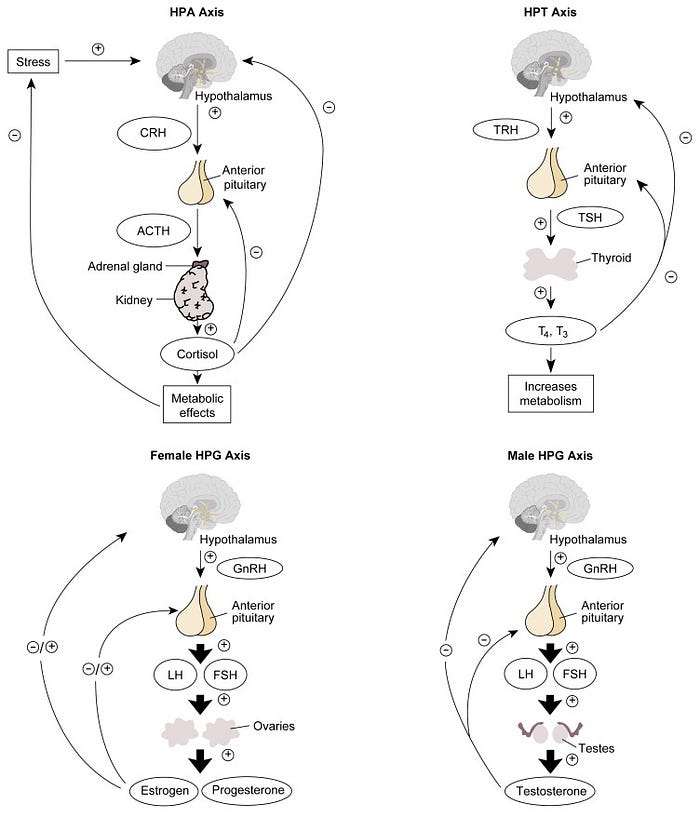
The HPA Axis
- Activation of the HPA axis, which regulates various metabolic functions, is initiated with the release of CRH from the hypothalamus. This release occurs in response to various stimuli, including almost any type of physical or psychological stress; during the normal sleep-wake cycle; and in response to certain neurotransmitters. CRH then stimulates the anterior pituitary to produce ACTH. (In addition to CRH, AVP from the hypothalamus also can stimulate ACTH release). ACTH, in turn, activates adrenal hormone production, primarily of cortisol, which mediates the specific physiological effects of this hormone system.
- The activity of the HPA axis is regulated by negative feedback mechanisms. Thus, increased cortisol levels repress CRH release by the hypothalamus and ACTH release by the pituitary. In addition, ACTH can directly inhibit hypothalamic CRH release.
- Any disturbances in the HPA axis can result in serious medical consequences. For example, insufficient hormone production by the adrenal cortex causes Addison’s disease, which is characterized by muscle weakness, dehydration, loss of appetite (i.e., anorexia), nausea, vomiting, diarrhea, fever, abdominal pain, tiredness, and malaise. Patients with this disease exhibit low levels of plasma cortisol but high levels of ACTH. The increase in ACTH levels represents a vain attempt by the pituitary to stimulate hormone production in the unresponsive adrenal cortex.
- Equally deleterious is the excessive glucocorticoid production that results from excess ACTH release (i.e., Cushing’s syndrome). Those patients experience symptoms such as muscle weakness and wasting, back pain from osteoporosis, a tendency to bruise easily, redistribution of body fat (i.e., a rounded “moon” face, prominent abdomen, and thin legs), and various psychological disturbances. Because of the negative feedback mechanism of the HPA axis, the patient’s cortisol levels are high and the ACTH levels are low.
- Both acute and chronic alcohol consumption have been shown to activate the HPA axis, and some drinkers develop a so-called pseudo-Cushing’s syndrome that disappears with abstinence.
The HPG Axis
- In both men and women, the HPG axis is the hormone system that controls the release of sex hormones. In both genders, the system is activated by GnRH, which is released regularly in short bursts from the hypothalamus. GnRH then stimulates the release of FSH and LH from the anterior pituitary.
- In men, LH stimulates certain cells in the testes (i.e., Leydig cells) to release testosterone. FSH and testosterone are key regulators of another set of testicular cells (i.e., Sertoli cells), which support and nourish the sperm cells during their maturation. The HPG axis in men is regulated through a variety of factors. For example, testosterone is part of a negative feedback mechanism that inhibits GnRH release by the hypothalamus and LH release by the pituitary. In addition, the Sertoli cells secrete a substance called inhibin, which prevents FSH release from the pituitary. Finally, the Leydig cells and, to a lesser extent, the Sertoli cells produce a substance called activin, which stimulates FSH secretion and thus has the opposite effects of inhibin.
- In women, during the menstrual cycle, LH and FSH stimulate the ovarian follicle that contains the maturing egg to produce estradiol. After ovulation has occurred, LH also promotes production of progesterone and estradiol by the corpus luteum. Both hormones participate in a negative feedback mechanism through most of the menstrual cycle, suppressing GnRH release from the hypothalamus and LH release from the pituitary. Shortly before ovulation, however, a positive feedback mechanism is activated by which estradiol actually enhances LH release from the pituitary. The resulting surge in LH levels ultimately leads to ovulation, the formation of the corpus luteum, and progesterone release. Progesterone exerts a negative feedback on LH and FSH release, causing LH levels to decline again. In addition to those mechanisms, FSH release from the pituitary is regulated by inhibin, a substance produced by certain cells in the ovarian follicle.
- Both acute and chronic alcohol consumption can interfere with the normal functioning of the HPG axis, resulting in reduced fertility or even infertility in both men and women and in menstrual disturbances in women.
The HPT Axis
- The hormones that make up the HPT axis control the metabolic processes of all cells in the body and are therefore crucial for the organism to function normally. The secretion of TRH from the hypothalamus activates the HPT axis. After reaching the pituitary, TRH stimulates the release of TSH, which in turn promotes the production and release of T 4 and T 3 by the thyroid gland. Negative feed-back effects of T 4 and T 3 on both the hypothalamus and the pituitary regulate the HPT system.
Alcohol’s Effects on the Hypothalamic-Pituitary-Thyroid Axis
- One of the essential hormonal systems regulating normal body functioning is the hypothalamic-pituitary-thyroid (HPT) axis, which controls the metabolism of all cells. As with other hormone systems, alcohol consumption under certain conditions can modify the release of hormones involved in this axis. In healthy nonalcoholics, alcohol consumption does not appear to induce any significant changes in the HPT axis. Conversely, some effects of alcohol on the HPT axis have been observed in alcoholics. The effects differ depending on the drinking status of the alcoholics studied. In alcoholics undergoing withdrawal, baseline levels of thyroid hormone (i.e., T 3 and T 4) in the blood differ only minimally from those in nonalcoholics. The ability of hypothalamic thyrotropin-releasing hormone (TRH) to activate the release of thyroid-stimulating hormone (TSH) from the pituitary, however, is impaired in these alcoholics. This “blunting” effect may result from alcohol’s influence on the neurotransmitter dopamine. Dopamine produced in the hypothalamus acts not only as a neurotransmitter but also as a hormone in that it inhibits the release of both TSH and prolactin from the pituitary. Alcohol has been shown to increase dopaminergic activity and thereby may suppress the TSH response to TRH. This hypothesis is supported by the fact that prolactin release in response to TRH also is blunted in alcoholics undergoing withdrawal.
- Alcohol’s effects on the HPT axis are even more complex in abstinent alcoholics. In those people, the baseline levels of T 3 and sometimes T 4 are lower than in nonalcoholics. It is unclear, however, if this change represents a direct effect of long-term alcohol consumption or results from co-occurring alcohol-related illnesses, because thyroid hormone levels are often reduced in patients with acute or chronic non-thyroid-related illnesses, such as sepsis, burns, or major trauma. In addition to the reduced thyroid hormone levels, however, the TSH response to TRH remains blunted in abstinent alcoholics, whereas the prolactin response to TRH has returned to normal levels. This observation indicates that a factor other than dopamine likely contributes to this effect, although the exact mechanisms are unknown.
- Finally, some intriguing findings have suggested that abnormal responses of the HPT axis may represent a marker for a person’s vulnerability to alcoholism. Thus, some people who are at high risk for developing alcoholism, such as nonalcoholic sons of alcoholic fathers, tend to exhibit a blunted TSH response to TRH . These observations still require further investigation, however, for researchers to fully understand their significance.
Summary
- The neuroendocrine system is a highly complex and tightly controlled network of hormones released by endocrine glands throughout the body. The levels of some of the hormones are regulated in a fairly straightforward manner by the end products that they influence. Thus, blood sugar levels primarily regulate insulin and glucagon release by the pancreas. Other hormones (e.g., those of the HPA, HPG, and HPT axes) are parts of hormone cascades whose activities are controlled through elaborate feedback mechanisms. In addition, numerous indirect interactions exist between the various hormone systems governing body functioning. For example, hormones such as GH and thyroid hormone, through their effects on cellular metabolism, may modify blood sugar levels and, accordingly, insulin release.
Immunity and the Endocrine System
- The immune system is highly receptive to endocrine signals due to the expression of hormone receptors on immune cells. The impact of this immune–endocrine cross talk and related immune responses becomes clearly evident when assessing immunity from a sex-specific perspective. We here describe the effect of hormones, primarily sex- and stress-related steroid hormones, on cells of the innate and adaptive immune system in men and women. We specify how these effects are operational throughout the life span and also during periods of dramatic hormonal changes, such as pregnancy.
- The immune system actively maintains immune homeostasis by preventing immune reactions against self-antigens and eliminating pathogens. Interestingly, the immune system is also highly receptive to signals from other systems of the body, such as the endocrine system. This immune-endocrine cross talk is possible due to the expression of hormone receptors on a wealth of immune cells. Vice versa, endocrine tissues have been shown to be responsive to immune mediators, such as cytokines.
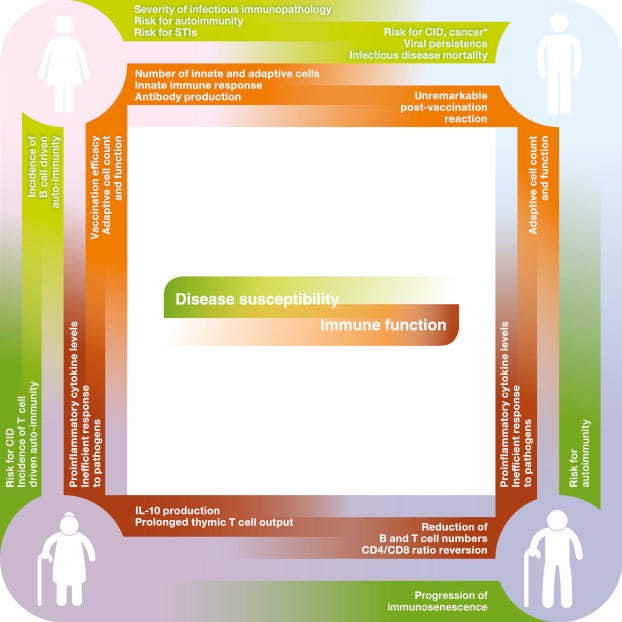
- The significant impact of hormones on the immune system becomes evident in the differential susceptibility to and progression of diseases that can be observed in men and women , mirrored by, for example, a higher incidence of autoimmune diseases and sexually transmitted infections (STIs) in females compared to males. These epidemiological observations suggest that respective sex-specific hormone concentrations account for the sex-specificity of immunity especially in adult humans (figure 1 ).

- Further, senescence of the endocrine system in the aging individual is paralleled by changes of the susceptibility to infectious diseases and, again, occurs differently in females and males . During their waning years, men show, for example, an increased mortality related to infections with human immunodeficiency virus (HIV), toxoplasmosis, and measles , while women experience a higher susceptibility and mortality to, for example, hepatitis, tetanus, leptospirosis, meningococcal, and pneumococcal infections, especially after menopause.
- Endocrine modulation of immunocompetence is not only apparent between the sexes. Intrafemale hormone levels vary tremendously throughout the reproductive cycle to ensure ovulation, fertilization, and implantation, while endocrine adaptations during pregnancy are necessary to promote successful growth of the fetus and dampen the risk of rejecting the semiallogeneic fetus. Hormonal changes occurring during the stages of the menstrual cycle as well as during pregnancy are associated with alterations in female immunocompetence.
- In this review, the sex- and age-specific effects of endocrine-immune cross talk on innate, antigen-presenting, and adaptive immune cells will be highlighted. A focus is given on steroid hormones (estrogens, progesterone, testosterone, glucocorticoids (GCs)), as the effect of these hormones is best understood to date. It should be noted that immune modulation by hormones responsible for growth and metabolism , leptin , thyroid hormones ), fluid and electrolyte balance (e.g., vasopressin and the steroid hormone aldosterone), as well as norepinephrine (noradrenaline), and epinephrine (adrenaline) can also affect immunity. The interested reader is referred to cited articles or related chapters in the present book.
Endocrine Modulation of Immunocompetence
- Release of sex and stress steroid hormones from endocrine glands is controlled by pathways, so called axes, which originate in the brain and signal to peripheral endocrine organs of the body ( figure 2).

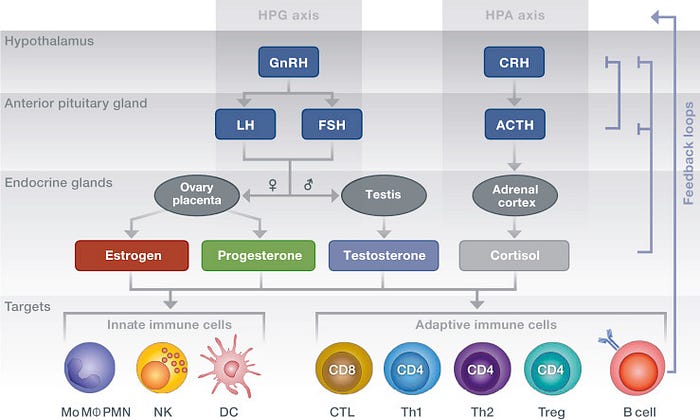
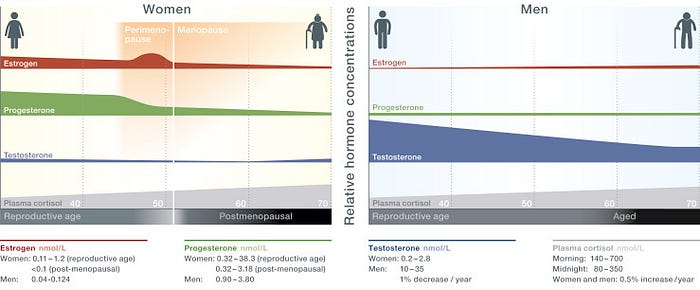
- Reproductive functions in females are regulated by key female sex hormones, such as estrogens and progesterone. The key male sex hormone is testosterone, which belongs to the group of androgens. In both sexes, cortisol, a GC, is the major hormone secreted in response to stress signals. The levels of these hormones are altered significantly over a human life span and differ between females and males in relation to age ( figure 3).

- Steroid hormones bind to specific hormone receptors (which are either nuclear or membrane bound) and induce both genomic and nongenomic actions in resident and circulating immune cells . A summary of these effects on distinct cell subsets of both the innate and adaptive immune response, is depicted in figure 4 and detailed below.

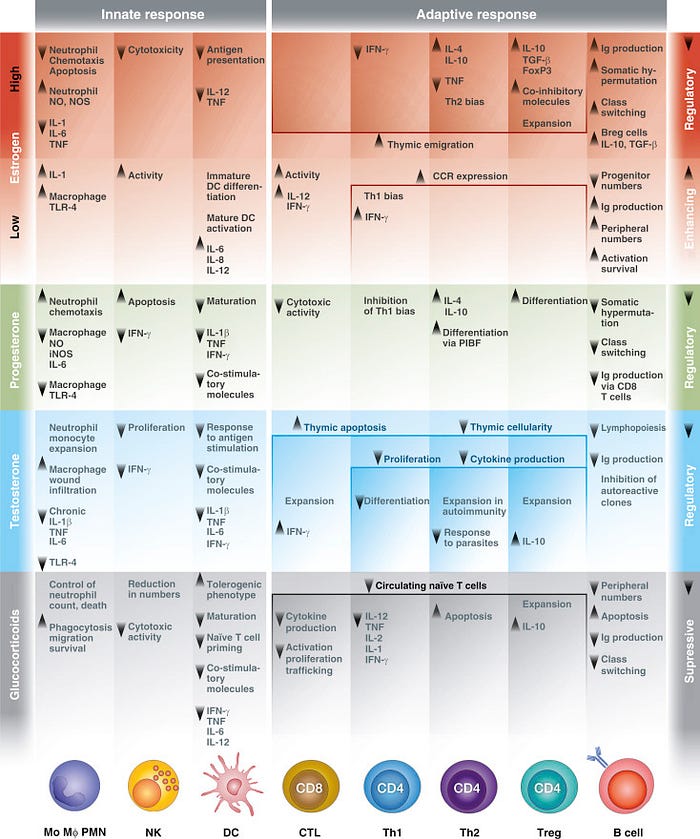
Estrogens
- The effect of estrogens on immune cells depends on their concentrations. Estrogen levels are considerably low during the early secretory and early postovulatory phase of the menstrual cycle as well as after menopause, whereas estrogen levels elevate to high levels during the late follicular phase prior to ovulation and further upsurge during pregnancy.
- Low estrogen levels stimulate cells of the innate immune response . Conversely, high concentrations of estrogens contribute to the repression of proinflammatory innate functions and suppress efficient dendritic cell (DC) antigen presentation.
- Estrogens also affect the adaptive immune response, for example, at the primary site of T cell generation in the thymus. Here, estrogens can induce thymic atrophy , increase the generation of mature CD4+T cells, and their emigration . One striking estrogen-mediated feature is the concentration-dependent effect on CD4+T helper (Th) cell polarization: low concentrations of estrogens are paralleled by Th1 cell proliferation, cell-mediated immunity, and interferon (IFN)-γ as well as antibody production. This response is of rather proinflammatory nature and accompanied by increased cytotoxic CD8+T lymphocyte (CTL) activity. Conversely, high-estrogen concentrations increase interleukin (IL)-4 production by Th2 cells, which induce humoral immunity and have an anti-inflammatory effect. High levels furthermore expand regulatory T (Treg) cells , accompanied by an increased expression of IL-10 and transforming growth factor β , inhibitory costimulatory molecule programmed cell death protein (PD)-1 , and cell death-mediating perforin.
- Although estrogens decrease B cell progenitors in the bone marrow , they increase the number of peripheral B cells , their activation, maturation, and survival , and production of antigen-specific antibodies .
- Overall, the effects on estrogens on the immune system can be summarized as immunoenhancing due to the stimulation of innate immune cell function, CTL activity, and Th1 responses as well as antibody production and B cell maturation. This effect is considered to contribute to the relative immunological advantage of females in mounting an immune response toward pathogens.
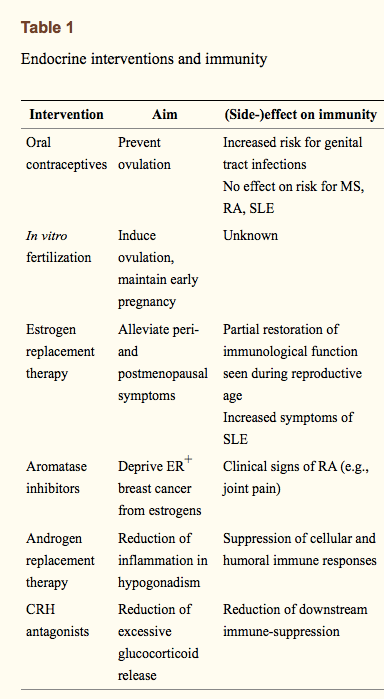
Progesterone
- Progesterone downregulates innate immune responses exerted by macrophages , natural killer (NK) cells , or DCs . Further, progesterone antagonizes the effect of estrogens on T cell cycle progression and apoptosis and inhibits proliferation of T cells after DC stimulation and their differentiation into proinflammatory Th17 cells. Most importantly, the high concentrations of progesterone present during pregnancy inhibit a Th1 bias of the immune response by stimulating the generation of Treg cells and anti-inflammatory, IL-4- and IL-10-secreting CD4+Th2 cells. Moreover, progesterone decreases immunoglobulin-secreting B cell numbers and suppresses their maturation.
- Hence, the overall effects of progesterone can be summarized as immunosuppressive.
Testosterone
- Testosterone supports the innate immune response by enhancing neutrophils . While testosterone supports the production and function of actively patrolling monocytes/macrophages , it suppresses macrophage function in chronic inflammation , dampens their sensitivity to recognize pathogenic patterns , and suppresses NK cell proliferation. DCs are suppressed by testosterone via inhibition of costimulatory molecule expression, a reduced proinflammatory cytokine production and a diminished antigen-responsive capacity .
- The adaptive immune response is also suppressed by testosterone, mirrored by a reduced T cell proliferation and cytokine production , a lower proliferation of immature thymocytes, and accelerated thymic apoptosis , thereby inducing thymic atrophy . Testosterone inhibits Th1 differentiation ), IFN-γ secretion in NKT cells , and parasite-induced Th2 responses . In turn, it enhances Th2 immunity to counteract overshooting Th1 responses in autoimmunity and induces expansion of suppressor CD8+cells and Tregs . B cell proliferation and immunoglobulin production are reduced in response to androgens .
- Overall, testosterone exerts immune-suppressive effects on the immune response, which has been suggested to protect males from autoimmunity.
Glucocorticoids
- Cortisol, along with the other endogenous GCs, have a dichotomous effect on the innate immune response, as they stimulate macrophages , but repress NK cells . Also, GCs inhibit DC maturation and antigen-presenting function , thereby locking DCs in a tolerogenic state . With regard to the adaptive immune response, GCs reduce the levels of circulating naïve T cells and trigger T cell apoptosis . They suppress CD8 T cell activation, proliferation, and trafficking and reduce NKT cell number and cytotoxic activity . GCs suppress cellular (Th1) immunity by repressing production and release of Th1 and Th17 proinflammatory cytokines and favor humoral (Th2) immunity . In turn, the differentiation of IL-10-producing Tregs is promoted . B cells are repressed by GCs .
- To summarize, GCs are rather strong immune-suppressors, an effect which is therapeutically utilized to dampen inflammatory symptoms in many diseases by exogenous supplementation of synthetic GCs.
- Noteworthy, besides the direct effects of hormones on the immune system discussed so far, steroid hormones can also indirectly affect immunity. For example, estrogens contribute to recruitment of inflammatory cells via the upregulation of adhesion molecules on endothelial cells . Testosterone strengthens tight junctions of the blood-testis barrier , thereby supporting the immune privilege of the testis.
- We here refrain from discussing reciprocal effects of the immune system on the endocrine system, such as the effect of cytokines on key endocrine tissues, like the hypothalamus, pituitary gland, or thyroid .
Consequences of Endocrine-Immune Cross Talk
Sex Disparity of Adult Immune Responses
- Most of the described immune-endocrine effects described above and depicted in are compiled from observations in different species, cell subsets from different organs, from distinct disease models, or from in vitro experiments. Hence, it is difficult to appreciate the biological consequences of these cross talks between hormones and immune cells. Epidemiological observations greatly facilitate understanding of the implications of immune-endocrine interaction for health and disease ( and ). Here, the more readily initiated innate immune response to pathogens and a more efficient antigen presentation seen in females could be attributed to the predominance of estrogens , which promotes the response to infections, vaccination, and trauma with a stronger adaptive response of Th1 cell-mediated immunity, along with Th2-triggered humoral immune responses . Females also exhibit higher immunoglobulin levels both at baseline and following infection or immunization, which promotes the elimination of viral pathogens . This health advantage related to immunity has significant collateral disadvantages, mirrored by the increased risk for autoimmunity in women. Here, the estrogen-induced promotion of T cell and B cell lymphopoiesis has been proposed to promote the escape from negative selection, hereby leading to the presence of autoreactive cells . The autoreactive cells can subsequently contribute to the etiology of rheumatoid arthritis (RA) , systemic lupus erythematosus (SLE) , Sjögren’s syndrome (), or multiple sclerosis (MS) .
- Conversely, the immunosuppressive effects of testosterone have been proposed to be advantageous in protecting males from autoimmunity. Indeed, testosterone has been shown to decrease the number of autoantibodies by inhibiting the expansion of autoreactive B cell clones . In accordance with this, declining levels of testosterone increase the risk for autoimmune diseases in males. Conversely, the testosterone-mediated immunosuppression also explains the increased viral persistence seen in men . Chronic immune diseases including atherosclerosis and metabolic diseases, such as type 2 diabetes, are also more prevalent among men. This health disadvantage has been attributed to the lack of estrogens, which can protect against vascular injury and atherosclerosis and regulate metabolic pathways . Another potential disadvantage related to immune-endocrine interaction is the overall higher risk of adult men to develop cancer, which has been linked to the testosterone-related dampened immune responses to neoplasms.
Sex-Based Senescence of the Immune Response
- Besides sex hormone-related differences in immunity, the age-associated decrease of estrogens and progesterone in women and testosterone in men can result in altered immune responses and risk for diseases ( and ). Indeed, female- and male-aged individuals show higher-serum levels of a proinflammatory cytokines, which has been termed inflammaging . Despite this inflammatory status, aging is characterized by a less-efficient innate defense against pathogens and a decreased functionality of the adaptive immune response . Treg cells and differentiated T cells with memory and effector functions accumulate in the periphery , which has been proposed to render the aged individual less flexible to fight novel pathogens and could explain the reduced vaccination efficacy in the aged of both sexes . Studies on sex-specific differences in immunosenescence are sparse, but the reduced levels of testosterone could allow for the increased occurrence of autoimmune diseases seen in aging males, while the decrease in estrogens reduces autoantibody-driven autoimmunity in females, while at the same time enhancing T cell-mediated autoimmune diseases . Future studies are needed to elucidate immune-endocrine mechanisms modulating the course of infectious diseases and vaccination efficacy in the elderly.
Steroid Hormones Affecting Immunity in Female Reproduction
Immunocompetence of the Cycling Female and the Window of Vulnerability
- Besides the immune-endocrine interactions discussed so far with regard to systemic immunity, fluctuations in hormone concentrations that occur over the relative short-time period of the menstrual cycle are associated with marked changes in the local immune response in the reproductive tract .

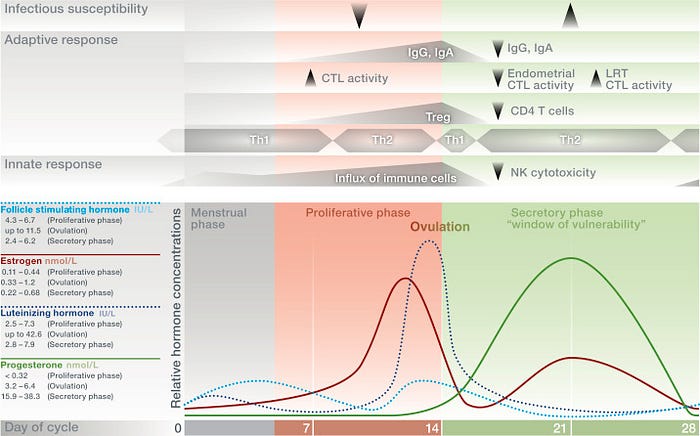
- Commencing in the late-secretory phase, immune cells in the uterine endometrium begin to increase and surge during the estrogen-rich proliferative phase. This cellular influx is increasingly facilitated with progressive formation of new vasculature and accumulation of chemokines and peaks at the time of ovulation, possibly to provide a receptive environment for blastocyst implantation. During ovulation, estrogens induce immunoglobulin secretion to facilitate removal of potential pathogens . Moreover, the increased number of Treg cells in the endometrium throughout the proliferative phase until ovulation points toward their possible role in promoting local immune tolerance to facilitate blastocyst implantation .
- During the secretory phase, both progesterone and estrogen levels are high, which dampens immunosurveillance and thereby minimizes the risk of an immune response against allogeneic sperm antigens and — if implantation occurs — the semiallogeneic blastocyst. This is accompanied by low-antibody levels in cervical secretions . At the same time, the endometrium prepares for a possible blastocyst implantation via an increase of uterine NK cells. These NK cells show a unique phenotype, as they exhibit low-cytotoxic activity . Additionally, endometrial CD8+cytotoxic T lymphocyte activity is suppressed. Surprisingly, after peaking around ovulation, Treg cell numbers decrease at the beginning of the secretory phase, which challenges their central role in contributing to persisting immune tolerance during very early pregnancy .
- The fluctuating levels of estrogens and progesterone during the menstrual cycle and the associated changes in immune function have been proposed to influence the response to mucosal pathogens. Studies performed in mice reveal a reduced protection from bacterial infection in the genital tract in response to progesterone . Also, viral infection appeared to be enhanced in dioestrus (corresponding to the secretory phase with high progesterone levels in humans), while viral replication was reduced during the estrogen-dominated preovulatory phase . Hence, a window for increased susceptibility to STIs, for example, HIV, has been proposed for the secretory phase of the menstrual cycle due to the suppression of innate, humoral, and cell-mediated immunity by progesterone and high estrogens . In conclusion, immunity in the female reproductive tract faces a contradictory demand by suppressing an immune response against allogeneic sperm antigens and promoting the implantation of a semiallogeneic blastocyst. This is at the expense of immunity against local pathogen challenges.
Immune Privilege of the Pregnant Uterus: Adaptations of Maternal Immunocompetence
Besides the endocrine changes occurring over the menstrual cycle, pregnancy is accompanied by soaring hormone levels (figure 6 ). These pregnancy-related hormonal changes skew the innate and adaptive immune response to contribute to a tolerogenic immune environment at the fetomaternal interface in which the fetus develops .

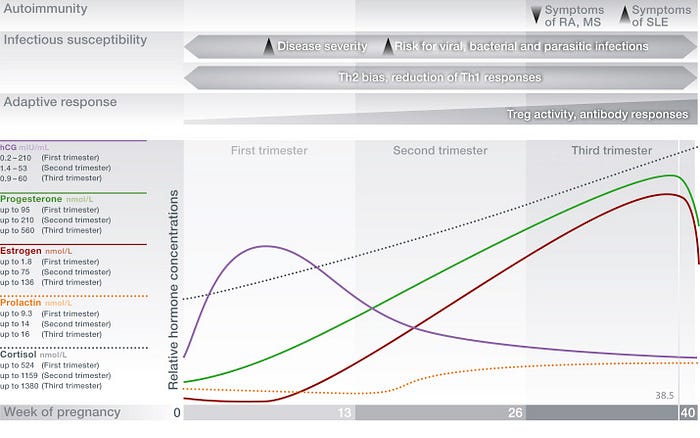
- Human chorionic gonadotropin drives the corpus luteum secretion of progesterone during early pregnancy and acts as a chemoattractant for decidual tolerogenic Tregs. The pregnancy-associated activation of the hypothalamic-pituitary-adrenal (HPA) axis increases immune-suppressive GC secretion, which is even further enhanced by placenta-derived corticotropin-releasing hormone, resulting in a protective hyporesponsiveness to stress at term pregnancy due to massive negative feedback . Levels of estrogens are high, exerting immune-regulatory functions (figure 4). The essential role of progesterone in maintaining a successful pregnancy becomes evident in observations in humans and mice that its reduction or blockage can result in fetal loss .
- While the maternal immune changes establish an immune privilege of the pregnant uterus to allow for fetal survival, the occurring systemic alterations have been shown to impair maternal immunity against pathogens and alter the activity of autoimmune diseases. The constantly rising levels of progesterone and the enhanced GC production in response to HPA-axis activation could increase the susceptibility to or severity of infectious diseases due to the suppression of a proper immune response necessary to control and eliminate pathogens. In pregnant mice, infection with Leishmania major, Salmonella enterica, and Toxoplasma gondii is more severe due to the suppressed Th1 immunity that would usually mount an antiparasitic response . Pregnant women are at an increased risk to suffer from acute and chronic viral infections such as rhinovirus, severe acute respiratory syndrome, coronavirus, varicella zoster, hepatitis E/B, HIV, and cytomegalovirus . Moreover, pregnant women are highly susceptible to influenza A virus infection, mirrored by the high incidence, morbidity, and mortality, as last observed by during the 2009 pandemic. This has been described to result from the contradictory demand for the immune system to mount a virus-specific immune response to clear the influenza infection, while simultaneously maintaining adaptation to pregnancy. Furthermore, antibody-mediated disorders such as SLE , sclerodermia , and thyroiditis are exacerbated during pregnancy, possibly due to enhanced antibody production in response to the high levels of estrogens.
- In contrast to these adverse effects of pregnancy on immunity, the immune-endocrine interaction during pregnancy can also be beneficial for maternal health. In female patients with MS or RA, both T cell-mediated inflammatory diseases, clinical symptoms have been reported to improve during pregnancy. This is followed by vigorous disease relapses shortly after parturition, when hormonal levels and immune adaptation are being restored to nonpregnancy levels . Strikingly, the amelioration of MS disease activity has been shown to exceed the effect size of currently available therapeutic strategies . Hence, a better understanding of underlying immune-endocrine pathways may provide insights for developing new treatments for these conditions .
Genetic Influence of Sex Chromosomes on Immune Response
- Noteworthy, the sex-specific endocrine response does not suffice to fully explain sex-specific immune responses. Investigations also aim to understand the genetic influence of the sex chromosomes on immune differences between the sexes. It has been proposed that the escape from X chromosome silencing and X inactivation skewing may reactivate parts of the second X chromosome in females, which could promote female immune function due to enhanced expression of immune-regulatory genes. Males, in contrast, have only one copy of the X chromosome which encodes for many genes involved in immunity . Also gender-related lifestyle factors may contribute to differential immunity and disease susceptibility.
Conclusion
- In this review, interactions of sex and stress steroid hormones with the innate and adaptive immune response have been discussed from a sex- and age-specific perspective and in certain settings, such as pregnancy. Additional evidence for the impact of hormones on the immune system can be observed during endocrine therapeutic interventions, which is listed in Table 1 . We highlight the biological consequences resulting from the interaction between hormones and immune cells in the context of health and diseases, as the current knowledge opens avenues for therapeutic interventions targeting pathways involved in the immune–endocrine cross talk, for example, during pregnancy complications or autoimmunity.